A New Era of Blood Clot Care — How CAVT Technology Could Democratize PE Treatment
March is Blood Clot Awareness Month and we are calling attention to meaningful progress in treating blood clot conditions like pulmonary embolism (PE).
PE care has seen delays in diagnosis and treatment disparities for years.1 Despite the emergence of advanced therapies, adoption has been slow due to gaps in evidence and a long learning curve. But emerging research suggests that we are entering a new era of blood clot care, one in which more patients could gain access to advanced therapies, with the goal to improve outcomes and save lives.
Penumbra Inc. is dedicated to innovating new therapies, like Computer Assisted Vacuum Thrombectomy (CAVT), which is designed to manage blood clots with speed, safety and simplicity. And we’re supporting scientific research to fill the evidence gap to bring these therapies to the patients who need them.
“Our focus at Penumbra has always been to create advanced technologies to help as many people as possible.” says Shruthi Narayan, President of Penumbra. “Our latest CAVT technology is designed to make thrombectomy fast and easy for clinicians, and safe for patients. And now we’re seeing the clinical evidence that it’s not just fast, it improves patient outcomes.”2,3
Awareness is Key
To ensure that all patients receive the blood clot care they need, patients and providers alike need to be aware of the risks. Up to 900,000 people are affected by venous thromboembolism (VTE) each year and up to 100,000 die annually by venous blood clots.4 VTE includes blood clots that form deep in the veins, usually in the legs, and PE, which occurs when a blood clot breaks off from the legs or arms and travels through the heart to the lungs, blocking blood flow. PE is a serious condition and can be life threatening, representing the third leading cause of cardiovascular death, and the majority of deaths from VTE.5
Most people don’t recognize the symptoms of PE — and it’s often not identified quickly enough by clinicians and first responders. When a PE obstruction strains the heart muscle, it has to work harder to push blood through the lungs. The symptoms can be subtle but often include shortness of breath, chest pain, rapid heartbeat, or even sudden collapse. PE is a medical emergency that can be fatal without prompt recognition and treatment.
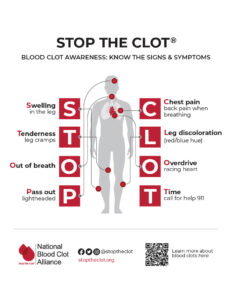
Know the Symptoms
The National Blood Clot Alliance — our partner in the Get Out the Clot Initiative — developed the STOP CLOT acronym to highlight the signs and symptoms of blood clots.
The Need for More Standardized Care
Many PE patients face delays or misdiagnosis, and unlike treatment for heart attack or stroke, care often varies greatly from hospital to hospital. A recent Get Out the Clot Survey found that only 56% of interventionalists surveyed believe their protocols provide clear direction based on PE risk beyond medical management, and approaches vary, even for patients with the same risk profile. And more than 50% of physicians surveyed say they do not have a formal response team at their institution, such as a pulmonary embolism response team (PERT) or a venous thromboembolism response team.
These inconsistencies underscore an urgent need for increasing public awareness, faster diagnosis, and standardized care paths. Everyone should know the symptoms of PE and seek immediate medical help when they occur. Once patients seek medical attention, they should be properly risk stratified to receive the right therapy at the right time.
Building Evidence for Advanced Therapy
The release of the landmark STORM-PE randomized controlled trial (RCT) results was a seminal moment in PE care. “This is a foundational trial that will significantly advance PE care, allowing these advanced therapies to be offered to more patients, improving patient outcomes, and potentially leading to the inclusion in future treatment guidelines,” said Dr. Robert Lookstein, MD, MSc; co-global principal investigator of the STORM-PE RCT and professor of radiology and surgery at Icahn School of Medicine at Mount Sinai.
STORM-PE Found CAVT Superior to Anticoagulation Alone
STORM-PE found that the use of CAVT with anticoagulation achieved superior reduction in right heart strain compared to anticoagulation therapy alone in patients with acute intermediate-high risk pulmonary embolism (PE), with a similar safety profile.2,a
The rate of major adverse events (MAE) within 7 days – including a composite of PE-related mortality, recurrent PE, clinical deterioration requiring rescue therapy, and major bleeding – was comparable between groups (4.3% [2/47] with CAVT vs. 7.5% [4/53] with anticoagulation alone).2
Further, the use of CAVT with anticoagulation achieved significantly greater improvements in thrombus burden reduction, heart rate, oxygen requirement, and functional outcomes compared to anticoagulation alone in patients with acute intermediate-high risk pulmonary embolism (PE).6
“Functional endpoints are critical because they capture outcomes that are most meaningful to patients,” said Dr. Rachel Rosovsky, MD, MPH, co-global principal investigator of STORM-PE RCT, hematologist at the Massachusetts General Hospital and Associate Professor of Medicine at Harvard Medical School. “Taken together the substantial improvement in RV function, early physiologic recovery, and superior functional outcomes provide a comprehensive assessment of the therapeutic benefit of CAVT in this patient population. These data can meaningfully inform shared decision-making when caring for patients with acute intermediate-high risk PE.”
How CAVT Technology Flattens the Endovascular Learning Curve
STORM-PE found CAVT to have a comparable safety profile to the current standard of care, anticoagulation alone. Achieving this safety profile with a new technology speaks to its ease of operation. That is a signal that CAVT technology may help flatten the learning curve and support the adoption of endovascular treatments across more hospitals.
And indeed, CAVT was engineered with simplicity in mind. Penumbra’s CAVT systems have refined algorithms designed to detect the difference between thrombus and patent flow. These devices provide real-time audio-visual cues alerting the operator when the clot is engaged for a more intuitive experience. These technological advances provide operators with an immediate and clear response to the changing dynamics of the procedure, designed to minimize the risk of complications and blood loss and optimize thrombus removal.
“Our ongoing innovation of our microprocessor algorithms and catheter technology aims to provide an improved physician experience and more efficient clot removal,” said Narayan. “This technology helps simplify a complex procedure allowing more hospitals to offer advanced therapies so more patients can benefit from them.”
Realizing System-Wide Benefits
Another new study analyzing real-world data found that the use of CAVT for intermediate-risk pulmonary embolism (PE) may shorten length of hospital stay, reduce complications, and improve discharge outcomes without increasing mortality compared to other treatment modalities.7 The research suggests that CAVT has the potential to help reduce healthcare costs. Other recent research has found similar benefits for CAVT use in lower extremity venous thrombus and acute limb ischemia.8,9
“CAVT provides physicians a safe and effective treatment for patients with severe symptomatic PE,” said James F. Benenati, M.D., FSIR, chief medical officer at Penumbra. “Data is now available demonstrating that this technology is superior to traditional anticoagulation for treatment of these patients. By increasing patient access to this technology we can improve patient outcomes while providing the healthcare systems with the benefit of reducing resource utilization, shortening lengths of stay, and ultimately decreasing costs.”8
Penumbra’s CAVT technologies allow physicians to address PE patients’ right heart strain due to PE faster and more completely than the traditional therapy. The system’s audio-visual cues make it easier and safe to implement in more hospitals. And CAVT’s positive impact on resource utilization may make it easy to scale across systems. Together, these benefits mark a new era of blood clot care — and begin the democratization of PE care by bringing advanced therapies to more patients who need it.
To learn more about CAVT and PE, subscribe here.
Important Safety Information
Additional information about Penumbra’s products can be located on Penumbra’s website at: https://www.penumbrainc.com/products/peripheral-thrombectomy-cavt/. The clinical results presented herein are for informational purposes only, and may not be predictive for all patients. Individual results may vary depending on patient-specific attributes and other factors. Caution: Federal (USA) law restricts these devices to sale by or on the order of a physician. Prior to use, please refer to Instructions for Use (IFU) for complete product indications, contraindications, warnings, precautions, potential adverse events, and detailed instructions for use. For the complete Penumbra IFU Summary Statements, visit: peninc.info/risk. Please contact your local Penumbra representative for more information.
Copyright ©2026 Penumbra, Inc. All rights reserved. CAVT and Lightning Flash are registered trademarks or trademarks of Penumbra, Inc. in the USA and other countries. All other trademarks are the property of their respective owners.
a. STORM-PE was not powered to detect differences in safety.
1. Hendriksen JM; Koster-van Ree M; Morgenstern MJ; Oudega R; Schutgens RE; Moons KG; Geersing GJ; (2017, March). Clinical characteristics associated with diagnostic delay of pulmonary embolism in primary care: A retrospective observational study. BMJ open. P. 1.
2. Lookstein RA, Konstantinides SV, Weinberg I, Dohad SY, Rosol Z, Kopeć G, Moriarty JM, et al. Randomized Controlled Trial of Mechanical Thrombectomy With Anticoagulation Versus Anticoagulation Alone for Acute Intermediate‑High Risk Pulmonary Embolism: Primary Outcomes From the STORM‑PE Trial. Circulation. 2025;153(1). doi:10.1161/CIRCULATIONAHA.125.077232.
3. Moriarty JM, Schiro BJ, Dohad SY, et al. Periprocedural results and right ventricular outcomes of computer assisted vacuum thrombectomy treatment of acute pulmonary embolism: interim analysis of 300 patients from the STRIKE‐PE study. J Am Heart Assoc. 2025;14(17):e039975. doi:10.1161/JAHA.124.039975
4. Centers for Disease Control and Prevention. (2023, June). Impact of Blood Clots on the United States Infographic. National Center on Birth Defects and Developmental Disabilities (NCBDDD). Accessed March 11, 2026.
5. Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet. 2012 May 12;379(9828):1835-46. doi: 10.1016/S0140-6736(11)61904-1. Epub 2012 Apr 10. PMID: 22494827.
6. Presented by Rosovsky, R. Randomized controlled trial of mechanical thrombectomy with anticoagulation versus anticoagulation alone for acute intermediate-high risk PE: primary outcome, functional endpoints, and core lab findings from STORM-PE. Presented at: VIVA (Vascular InterVentional Advances) 2025; November 3, 2025; Las Vegas, NV, USA.
7. Patel PJ, Dohad SY, Moriarty JM, Rosovsky R, Channick R, Weinberg I. Healthcare Resource Utilization and Outcomes in Intermediate-Risk Pulmonary Embolism in the United States. Am J Cardiol. 2025;257:183-190
8. Desai K, Hoots G, Ryu RK, et al. Computer-assisted vacuum thrombectomy vs. anticoagulation for iliofemoral deep vein thrombosis management: a comparative analysis of hospital and post-hospital outcomes. Presented at: SIR (Society of Interventional Radiology) 2025; Nashville, TN.
9. Bailey C, Arslan B, Elmasri F, et al. Therapy outcomes and healthcare resource utilization in computer assisted vacuum thrombectomy vs. open embolectomy: the THRIVE study. Presented at VAM (Vascular Annual Meeting) 2025; New Orleans, LA.
Related Articles
-
Employee Spotlight: Gabriel M. Vieira
March 26, 2026 -
Penumbra Presents Results for STORM-PE and STRIKE-PE, Adding to a Growing Body of Evidence Backing CAVT
March 24, 2026 -
Case Study: Next-Generation Lightning Flash 3.0 Efficiently Clears Right-Sided PE and Lower Extremity Venous Thrombus
March 5, 2026 -
EVT Panel Discussion: Expert Perspectives on the Modern PE Landscape
March 2, 2026